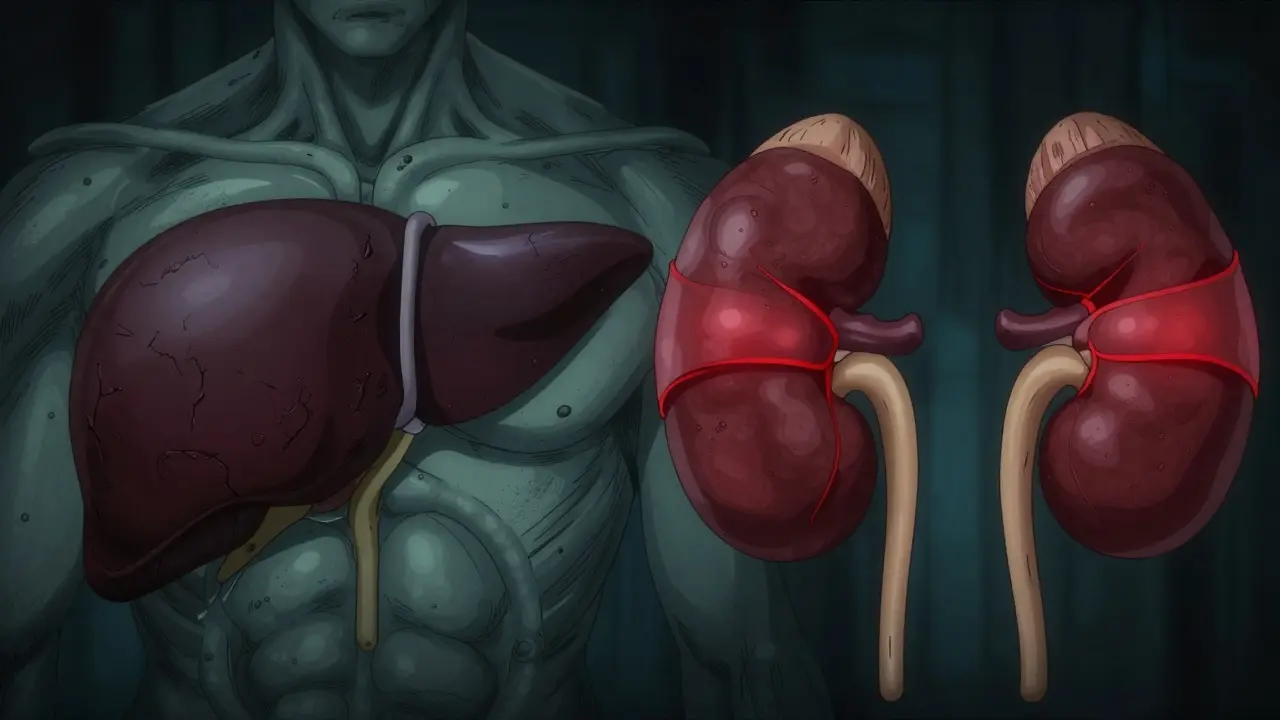
Imagine your liver is failing. It’s a terrifying prospect on its own. But for many patients with advanced cirrhosis, a severe scarring of the liver tissue that impairs function, the real danger isn’t just the liver-it’s what happens to the kidneys next. This condition is called Hepatorenal Syndrome (HRS), a life-threatening complication where the kidneys shut down not because they are damaged, but because the body’s circulation has gone haywire due to liver failure.
You might be wondering how healthy-looking kidneys can suddenly stop working. The answer lies in blood flow, not structure. In HRS, the kidneys themselves are physically intact. If you were to biopsy them, they would look normal. Instead, they fail because the blood vessels leading to them clamp down so tightly that blood cannot get through. It is a functional failure driven by the liver’s inability to regulate pressure and fluid balance. This distinction is crucial because it means the treatment isn’t about fixing the kidney tissue; it’s about reversing the circulatory crisis.
The Mechanics of Failure: Why the Kidneys Shut Down
To understand HRS, you have to look at the plumbing of the abdomen. When the liver becomes scarred from conditions like alcohol-related liver disease or viral hepatitis, blood faces resistance trying to pass through it. This creates high pressure in the portal vein, known as portal hypertension, increased blood pressure within the portal venous system.
This high pressure causes the arteries in the gut to widen (vasodilation). Blood pools in the belly, leaving less blood available for the rest of the body. Your brain senses this drop in effective blood volume and panics. It triggers emergency systems-the renin-angiotensin-aldosterone system (RAAS) and the sympathetic nervous system-to squeeze blood vessels tight to keep blood pressure up. The problem? The kidneys’ arteries are squeezed too. Renal blood flow can drop by 40-50%, causing the glomerular filtration rate (GFR) to plummet. The kidneys starve for oxygen and nutrients, even though there is plenty of fluid in the body-just not in the right place.
Type 1 vs. Type 2: Two Different Speeds of Crisis
Doctors classify HRS into two types based on how fast the kidney function declines. Knowing which type you or a loved one has determines the urgency of treatment.
| Feature | Type 1 HRS | Type 2 HRS |
|---|---|---|
| Progression | Rapid, progressive decline | Gradual, stable decline |
| Creatinine Level | Doubles to >2.5 mg/dL within 2 weeks | Between 1.5-2.5 mg/dL |
| Primary Association | Acute-on-chronic liver failure | Refractory ascites (fluid buildup) |
| Survival Without Treatment | Median of 2 weeks | Months to years |
| Urgency | Medical emergency | Requires monitoring and management |
Type 1 is the acute emergency. It develops over days. A patient’s serum creatinine-a waste product filtered by kidneys-shoots up quickly. Without intervention, median survival is just two weeks. Type 2 is slower. It often presents as stubborn fluid accumulation in the abdomen (ascites) that doesn’t respond to standard diuretics like spironolactone or furosemide. While less immediately fatal than Type 1, it still signals advanced disease and carries a poor prognosis without transplant evaluation.
Diagnosing the Invisible Problem
Because the kidneys look normal under a microscope, diagnosing HRS is largely a process of elimination. Doctors must rule out other common causes of kidney injury, such as dehydration (prerenal azotemia), direct toxin damage (acute tubular necrosis), or blockages (obstructive uropathy).
According to the 2022 criteria from the International Club of Ascites (ICA), a diagnosis of HRS requires specific markers:
- No improvement after volume expansion: Giving 1g/kg of intravenous albumin for two days does not lower creatinine levels.
- Low urine sodium: Less than 10 mmol/L, indicating the kidneys are desperately holding onto salt.
- High urine osmolality: Greater than plasma osmolality, showing the kidneys are concentrating urine to save water.
- No significant protein or blood: Absence of heavy proteinuria (>500 mg/day) or hematuria (>50 red blood cells per field), which would suggest structural kidney disease.
Misdiagnosis is common. Studies show that 25-30% of HRS cases are initially misidentified, leading to inappropriate treatments. For example, giving more fluids to someone with HRS can worsen ascites and breathing difficulties, while withholding necessary vasoconstrictors delays life-saving care.

Treatment Options: From Drugs to Transplants
If you suspect HRS, time is critical. The goal is to reverse the vasoconstriction in the kidneys and buy time for a definitive solution.
Vasoconstrictors and Albumin
The current gold standard for Type 1 HRS involves combining terlipressin, a synthetic vasopressin analog that constricts splanchnic blood vessels with intravenous albumin. Terlipressin redirects blood away from the gut and back to the systemic circulation, relieving the pressure on the kidneys. In the pivotal CONFIRM trial, 44% of patients achieved renal recovery (creatinine dropping below 1.5 mg/dL) within 14 days.
In regions where terlipressin is unavailable or unaffordable, doctors may use a combination of midodrine and octreotide, though evidence supports these as second-line options. Albumin helps expand plasma volume and prevents further shock. Typical dosing starts with 1g/kg on day one, followed by 20-40g daily.
TIPS Procedure
For some patients, particularly those with Type 2 HRS and refractory ascites, a Transjugular Intrahepatic Portosystemic Shunt (TIPS), a procedure creating a channel between the portal and hepatic veins to reduce pressure can be effective. TIPS lowers portal hypertension directly, improving kidney perfusion. However, it carries risks, including a 30% chance of worsening hepatic encephalopathy (brain fog/confusion due to toxins). It is generally reserved for patients who are good candidates for future transplantation.
Liver Transplantation
Ultimately, HRS is a symptom of end-stage liver disease. Medications can stabilize kidney function, but they do not cure the underlying liver failure. Liver transplantation, the surgical replacement of a diseased liver with a healthy one remains the only definitive cure. Data from the United Network for Organ Sharing (UNOS) shows that 1-year survival after transplant for HRS patients is 71.3%, compared to just 18.2% with supportive care alone. Because of this, early listing for transplant is critical, even if kidney function hasn’t fully recovered yet.
Triggers and Prevention Strategies
HRS rarely appears out of nowhere. In nearly 70% of cases, there is a precipitating event that tips the balance. Identifying and treating these triggers can sometimes prevent full-blown HRS or reverse early stages.
- Spontaneous Bacterial Peritonitis (SBP): An infection of the abdominal fluid. This is the most common trigger (35% of cases). Immediate antibiotic therapy is essential.
- Gastrointestinal Bleeding: Upper GI bleeds from varices cause sudden blood loss and circulatory collapse.
- Large Volume Paracentesis: Removing large amounts of ascitic fluid without replacing albumin can lead to circulatory dysfunction.
- Nephrotoxic Drugs: NSAIDs (like ibuprofen or naproxen) and certain antibiotics can worsen kidney constriction. Patients with cirrhosis should avoid NSAIDs entirely.
Prevention focuses on aggressive management of ascites, prompt treatment of infections, and avoiding medications that stress the kidneys. Regular monitoring of creatinine and electrolytes in hospitalized cirrhotic patients is vital.

Living with the Diagnosis: Real-World Challenges
Beyond the physiology, HRS poses significant logistical and emotional hurdles. Access to terlipressin varies wildly by region. In the US, FDA-approved terlipressin (Terlivaz) became available in late 2022, but costs around $1,100 per vial, totaling over $13,000 for a standard course. Insurance denials are common, delaying treatment during a critical window.
Patient reports highlight the physical toll. Side effects of vasoconstrictors include severe abdominal pain, ischemia (reduced blood flow to limbs or heart), and arrhythmias. One patient noted needing dose reductions due to pain, while others described the anxiety of waiting for transplant lists to move. The Global Liver Institute found that 78% of HRS patients experienced diagnostic delays averaging over seven days, underscoring the need for better awareness among non-specialist physicians.
Future Directions and Hope
Research is active in this space. New biomarkers like urinary neutrophil gelatinase-associated lipocalin (NGAL) are being studied to detect HRS earlier, before creatinine rises significantly. Clinical trials are exploring novel vasopressin receptor agonists and devices to manage ascites more effectively. While challenges remain, the integration of standardized protocols in academic centers has already improved 30-day survival rates by 22%. Early recognition and rapid access to specialized care continue to be the strongest predictors of positive outcomes.
Is Hepatorenal Syndrome reversible?
Yes, in many cases, kidney function can be partially or fully reversed with timely treatment using vasoconstrictors like terlipressin and albumin. However, the underlying liver disease remains, making liver transplantation the only permanent cure for the syndrome itself.
What is the difference between HRS and regular kidney failure?
In regular kidney failure (like acute tubular necrosis), the kidney tissue is physically damaged. In HRS, the kidneys are structurally normal but fail due to severe constriction of blood vessels supplying them, caused by circulatory changes from liver disease.
Can I take painkillers if I have cirrhosis?
You should avoid NSAIDs (ibuprofen, naproxen, aspirin) as they constrict blood vessels in the kidneys and can trigger or worsen HRS. Acetaminophen (Tylenol) is generally safer in limited doses (up to 2g/day) but should always be discussed with your hepatologist.
How long can you live with Type 1 HRS without treatment?
Without treatment, the median survival for Type 1 HRS is approximately two weeks. It is considered a medical emergency requiring immediate hospitalization and intervention.
Does dialysis help with Hepatorenal Syndrome?
Dialysis is not a cure for HRS because it does not address the underlying circulatory issue. It may be used temporarily to manage complications like high potassium or fluid overload while waiting for vasoconstrictor therapy to work or for a liver transplant.
What triggers Hepatorenal Syndrome?
Common triggers include spontaneous bacterial peritonitis (abdominal infection), gastrointestinal bleeding, large-volume paracentesis without albumin replacement, and the use of nephrotoxic drugs like NSAIDs.
Is terlipressin available everywhere?
Availability varies. It is widely used in Europe and Asia. In the US, FDA-approved terlipressin (Terlivaz) became available in late 2022, but access can be limited by cost and insurance coverage. Other vasoconstrictor combinations may be used as alternatives.
Can TIPS cure HRS?
TIPS can improve kidney function in some patients, particularly those with Type 2 HRS and refractory ascites, by reducing portal pressure. However, it carries risks like hepatic encephalopathy and is not suitable for all patients. It is often a bridge to transplantation rather than a standalone cure.




Callie Skipper June 14, 2026
honestly this is just another way for the medical industrial complex to scare people into paying more for liver transplants which cost a fortune and still dont guarantee youll live forever lol
Miranda River June 16, 2026
Look, I have read this article and while it seems informative at first glance there are several glaring omissions that any true scholar of hepatology would immediately point out. The author fails to adequately address the nuanced interplay between the renin-angiotensin system and the sympathetic nervous system in a manner that reflects the latest peer-reviewed studies from the last six months specifically. Furthermore the distinction made between Type 1 and Type 2 HRS is overly simplistic and does not account for the emerging subtype classifications proposed by recent European societies of gastroenterology. It is also worth noting that the mention of terlipressin as a gold standard is somewhat dated given the ongoing trials with novel vasopressin analogs that show promising results in reducing ischemic side effects without compromising renal perfusion pressure. The article also neglects to discuss the role of gut microbiome dysbiosis in exacerbating portal hypertension which is a critical factor often overlooked in mainstream medical literature. Additionally the statistical data provided regarding survival rates lacks context regarding comorbidities such as diabetes or cardiovascular disease which significantly alter prognosis outcomes. One must also consider the socioeconomic disparities in access to care which are barely touched upon despite being a major determinant of patient survival in developing nations. The use of colloquial language like 'plumbing' undermines the scientific rigor expected in such a serious medical discussion and trivializes the complex pathophysiology involved. Moreover the section on triggers mentions NSAIDs but fails to elaborate on the specific mechanisms of prostaglandin inhibition leading to afferent arteriole constriction which is crucial for understanding why these drugs are so detrimental. The table comparing Type 1 and Type 2 is useful but could benefit from including data on urine output trends which are often more indicative of early decline than creatinine levels alone. It is also disheartening to see no mention of the psychological burden on caregivers who are left to navigate this bureaucratic nightmare of insurance denials and specialist referrals while their loved ones deteriorate. The reference to the CONFIRM trial is good but ignoring other conflicting studies creates a biased narrative that may mislead patients about the efficacy of treatment options available to them. In conclusion while the post serves as a basic overview it falls short of providing a comprehensive analysis that respects the intelligence of its readership and acknowledges the multifaceted nature of hepatorenal syndrome management.
Brandon Brodsky June 16, 2026
Sure because nothing says 'medical emergency' like a blog post written by someone who clearly hasn't spent time in an ICU watching kidneys fail in real time. The dramatic flair is unnecessary when the facts speak for themselves.
Ganesh Honikol June 18, 2026
I believe it is incredibly important to approach this topic with empathy and understanding because every individual's journey with liver disease is unique and deserves respect and compassion from the community. When we look at the physiological aspects described here such as the vasoconstriction of renal arteries due to splanchnic vasodilation we can appreciate the complexity of the human body and how interconnected our systems truly are which reminds us that health is not just about isolated organs but about holistic balance and harmony within ourselves. It is wonderful to see resources like this being shared because education empowers patients and families to ask better questions and advocate for themselves during difficult times when they might feel overwhelmed or confused by medical jargon and procedures. We should always remember that behind every statistic mentioned in this article there is a person struggling with fear uncertainty and hope and our role as a supportive society is to listen without judgment and offer encouragement rather than criticism or dismissal of their experiences. The information provided about terlipressin and albumin therapy is quite detailed and helpful for those seeking to understand current treatment protocols although it is essential to consult with healthcare providers before making any decisions regarding medication or procedural interventions such as TIPS or transplantation. I find it reassuring to know that research is ongoing and new biomarkers like NGAL are being studied which gives me hope that future treatments will be even more effective and less invasive for patients suffering from this devastating condition. Let us continue to support one another through these challenges by sharing knowledge and fostering a sense of community where everyone feels heard and valued regardless of their diagnosis or prognosis.
Emily Barnhill June 18, 2026
You need to stop spreading misinformation and realize that dismissing the severity of HRS based on your own biases is harmful to people who are actually suffering from this condition right now. If you think this is just about money then you clearly do not understand the life-threatening nature of acute kidney failure in cirrhosis patients and should educate yourself before commenting further.
Callie Skipper June 19, 2026
chill out emily nobody asked for your opinion anyway
Hailey Dunston June 21, 2026
It is quite amusing to observe how the masses flock to simplistic explanations of complex medical phenomena without questioning the underlying assumptions or considering alternative perspectives that might challenge the prevailing orthodoxy. The notion that terlipressin is the 'gold standard' is a testament to the pharmaceutical industry's influence on clinical guidelines rather than an objective assessment of therapeutic efficacy across diverse patient populations. One must wonder if the authors have considered the ethical implications of recommending expensive treatments that may not be accessible to all thereby perpetuating systemic inequalities in healthcare delivery. Furthermore the emphasis on liver transplantation as the only definitive cure ignores the potential for regenerative medicine approaches such as stem cell therapy or bioartificial livers which are currently under investigation and could revolutionize treatment paradigms in the near future. It is also pertinent to note that the psychological impact of receiving a diagnosis of HRS is profound and often underestimated by medical professionals who focus solely on physiological parameters while neglecting the emotional well-being of patients and their families. This holistic neglect contributes to a fragmented care model that fails to address the whole person resulting in suboptimal outcomes and diminished quality of life for those affected. Therefore it is imperative that we engage in critical discourse about the limitations of current practices and advocate for more inclusive and equitable approaches to managing hepatorenal syndrome.
AnneKatherine Stiekes June 22, 2026
i think its really sad how hard it is to get help sometimes especially when you are scared and alone but hopefully things will get better soon for everyone dealing with this