
When you hear the word biosimilar, you might think it’s just another name for a generic drug. But that’s not true. Biosimilars aren’t copies like generics-they’re highly similar versions of complex biologic drugs, made from living cells. The FDA doesn’t give them a star rating or a simple pass/fail. Instead, it uses a detailed, science-driven process to decide if a biosimilar is safe and effective enough to be approved. And understanding how this works matters-because it affects what treatments you can access and how much they cost.
How the FDA Approves Biosimilars
The FDA doesn’t treat biosimilars like traditional drugs. Biologics-like Humira, Enbrel, or Herceptin-are made from living organisms, which means no two batches are exactly alike. That’s why you can’t just reverse-engineer them like a pill. The FDA’s approval path for biosimilars was created by the Biologics Price Competition and Innovation Act (BPCIA) in 2010. It’s called the 351(k) pathway, and it lets companies skip doing all the big, expensive clinical trials that the original drug maker had to do.
But that doesn’t mean the FDA cuts corners. In fact, it’s the opposite. To get approved, a biosimilar must prove it’s highly similar to the reference product-with no clinically meaningful differences in safety, purity, or potency. That means if you switch from the original drug to the biosimilar, your body should react the same way. No extra side effects. No drop in effectiveness.
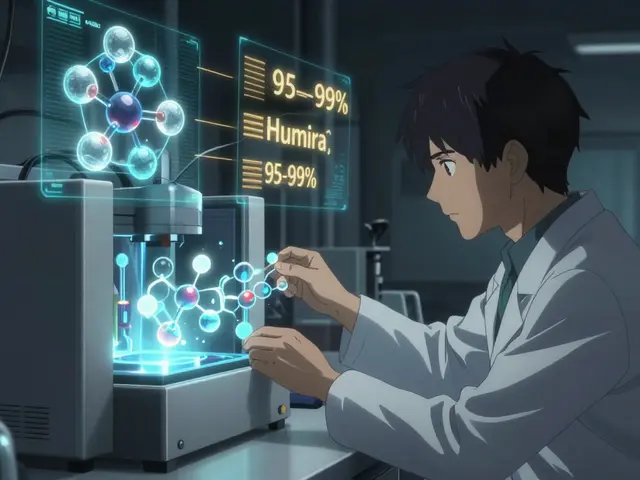
The process starts with lab tests. Developers use advanced tools like mass spectrometry and capillary electrophoresis to compare the molecular structure of the biosimilar and the original drug. They look at up to 300 different characteristics-things like protein folding, sugar attachments (glycosylation), and how the molecule binds to its target. The FDA expects 95% to 99% similarity across these attributes. If the data isn’t good enough, the application gets rejected before any human testing even begins.
Why Biosimilars Aren’t Generics
It’s easy to confuse biosimilars with generics, but they’re fundamentally different. Generics are exact copies of small-molecule drugs-like aspirin or metformin. Their chemical structure is simple and stable. You can make them in a lab using the same recipe every time.
Biosimilars? They’re made from living cells-usually bacteria or yeast. Tiny changes in the manufacturing process-temperature, pH, nutrient mix-can alter the final product. That’s why two batches of the same biologic drug from the same company can vary slightly. A biosimilar has to match that variability, not just a fixed chemical formula.
This complexity is why the FDA requires more data for biosimilars than for generics. A generic only needs to prove it releases the same active ingredient at the same rate. A biosimilar needs to prove it behaves the same way in your body-from how it’s absorbed to how your immune system responds.
The Role of the FDA Purple Book
If you want to know which biosimilars are approved and what they’re approved for, you check the FDA’s Purple Book. It’s not a physical book anymore-it’s a searchable online database updated daily. As of October 2025, it lists 43 approved biosimilars and 387 reference biologics.
The Purple Book doesn’t just list names. It shows which biosimilar matches which reference product. It includes patent information, exclusivity dates, and whether a product is designated as “interchangeable.” That last part is important.
An interchangeable biosimilar meets an even higher bar. It must show that switching back and forth between the original and the biosimilar won’t increase risk or reduce effectiveness. Only 17 of the 43 approved biosimilars have this status. Pharmacists can substitute them without needing a doctor’s approval-just like generics. The rest still require a prescription for the specific product.
How Clinical Studies Fit In
For years, the FDA required biosimilar makers to run full clinical trials comparing their product to the original. But that’s changing. In September 2024, the agency updated its guidance to allow companies to skip comparative clinical studies in many cases-if their analytical data is strong enough.
Now, most biosimilars only need one pharmacokinetic study in healthy volunteers. That’s usually a small trial with 50 to 100 people, measuring how fast the drug enters the bloodstream and how long it stays there. Sometimes, a pharmacodynamic study is added to check the drug’s effect on a biological marker, like how it lowers inflammation.
Immunogenicity testing is always required. That means checking whether the biosimilar triggers unwanted immune reactions-like antibodies that could neutralize the drug or cause allergic responses. These tests run for at least 24 weeks, sometimes up to a year.
Comparative efficacy trials (large studies showing the biosimilar works just as well in treating disease) are now the exception, not the rule. The FDA only requires them if there’s uncertainty about how the drug behaves in certain patient groups or if the molecule is especially complex.
Interchangeability: The Gold Standard
Not all biosimilars are created equal when it comes to substitution. Interchangeable biosimilars are the ones pharmacists can swap in without asking the doctor. To earn that label, the manufacturer must prove that switching between the reference product and the biosimilar multiple times doesn’t change the outcome.
That means running a study where patients are switched back and forth between the two products-say, four times over six months-and showing that safety and effectiveness stay the same. Only 17 biosimilars have cleared this hurdle as of late 2025.
For patients, this means fewer barriers. If your doctor prescribes a reference biologic and your pharmacy has an interchangeable biosimilar, you can get the cheaper version without a new prescription. For payers, it means faster cost savings.

Why So Few Biosimilars Have Launched
Even though the FDA has approved 43 biosimilars, only 29 have actually hit the market. Why? Patent lawsuits. Biologic drug makers often file multiple patents to delay competition, creating what’s called a “patent thicket.” A single biosimilar can face 20 or more legal challenges.
The average time from FDA approval to market launch is 11.3 months-mostly because of litigation. In oncology, biosimilars have moved faster. Drugs like rituximab and trastuzumab biosimilars now make up 65% to 75% of prescriptions within 18 months of launch.
But in autoimmune diseases like rheumatoid arthritis or Crohn’s, uptake is slower. Adalimumab biosimilars, approved in 2023, only reached 28% market share by mid-2025. Prescribers are hesitant. Payers don’t always push them. And some patients fear switching-even though data shows no safety issues.
Real-World Safety Data
Since the first biosimilar, Zarxio, was approved in 2015, the FDA has tracked safety through its Sentinel Initiative. As of Q3 2025, adverse event reports for biosimilars are statistically identical to those for the original biologics: about 0.8 per 10,000 patients for biosimilars versus 0.7 for reference products.
No biosimilar has shown a new safety signal. No increased risk of infection, cancer, or immune reactions. That’s backed by real-world data from millions of doses administered across the U.S.
Patients with cancer, autoimmune diseases, and chronic conditions have been using biosimilars for nearly a decade. The evidence is clear: they work. They’re safe. And they’re saving money.
What’s Next for Biosimilars
The FDA is working on new guidance for complex biosimilars-like antibody-drug conjugates and fusion proteins. Only three applications for these advanced products have been submitted so far. None have been approved.
In 2026, the agency plans to start using AI tools to analyze analytical data faster. It’s also developing a formal framework for interchangeable biosimilars of combination products-like insulin with a stabilizer-by 2027.
Industry experts predict approval rates will jump from 3-5 per year to 7-9 by 2027. Development timelines could shrink from nearly seven years to just over five. And if these changes stick, biosimilars could make up 30% of the U.S. biologics market by 2030-saving over $250 billion.
The path isn’t perfect. Manufacturing is still expensive. Regulatory hurdles remain. But the science is solid. The data is reassuring. And for patients who need life-changing biologics, biosimilars are no longer a hope-they’re a reality.
Are biosimilars the same as generics?
No. Generics are exact chemical copies of simple, small-molecule drugs. Biosimilars are highly similar versions of complex biologic drugs made from living cells. They can’t be identical because biological products naturally vary. Biosimilars require far more testing than generics to prove they work the same way in the body.
Does the FDA rate biosimilars like drugs on a scale of 1 to 5?
No. The FDA doesn’t assign ratings like A, B, or star scores. Instead, it makes a binary determination: either a biosimilar is approved as biosimilar or interchangeable, or it’s not approved at all. The decision is based on a full review of analytical, clinical, and manufacturing data-not a simple score.
What’s the difference between biosimilar and interchangeable?
All interchangeable biosimilars are biosimilars, but not all biosimilars are interchangeable. An interchangeable biosimilar has extra data proving that switching between it and the original product won’t increase risk or reduce effectiveness. Pharmacists can substitute interchangeable biosimilars without asking the prescriber-just like generics. Other biosimilars require a specific prescription.
How long does it take to get a biosimilar approved by the FDA?
The median time from initial application to approval is about 3.2 years. That’s longer than in Europe, mainly because the FDA requires more detailed analytical testing. For complex molecules, it can take longer-up to five or six years. The process includes analytical studies, animal testing (if needed), human pharmacokinetic studies, and immunogenicity monitoring.
Why are biosimilars cheaper than the original biologics?
Biosimilars cost less because they don’t need to repeat the massive clinical trials the original drug underwent. The FDA allows manufacturers to rely on the reference product’s safety and efficacy data. This cuts development costs by 30-50%. As a result, biosimilars typically cost 15-30% less than the original biologic, with some offering even deeper discounts once multiple competitors enter the market.
Can I be switched to a biosimilar without my doctor’s permission?
Only if the biosimilar is designated as “interchangeable” by the FDA and your state allows pharmacist substitution. For non-interchangeable biosimilars, your doctor must prescribe the specific product. Even with interchangeable products, some states require the pharmacist to notify your doctor after the switch.
Are biosimilars safe for long-term use?
Yes. Since Zarxio was approved in 2015, over 43 biosimilars have been used by millions of patients in the U.S. The FDA’s post-market surveillance shows no increased risk of serious side effects compared to the original biologics. Adverse event rates are nearly identical, and no new safety concerns have emerged over nearly a decade of real-world use.






Jane Lucas December 27, 2025
Biosimilars are a game changer. No more paying $20k for a drug that should cost $5k. This is healthcare finally making sense.
dean du plessis December 28, 2025
Interesting read. I never realized how complex biologics are compared to regular pills. The science behind this is actually pretty cool.
Raushan Richardson December 30, 2025
I’ve been on a biosimilar for RA for 2 years now. Same results, half the price. Why are people still scared? The data’s there.
John Barron December 31, 2025
The FDA’s 351(k) pathway is a masterclass in regulatory efficiency. By leveraging analytical comparability, they eliminate redundant clinical trials without compromising safety. The molecular characterization protocols-mass spectrometry, capillary electrophoresis, glycosylation profiling-represent a paradigm shift in pharmacovigilance. One must appreciate the rigor behind what appears on the surface to be a cost-cutting measure.
Miriam Piro January 2, 2026
They say biosimilars are safe... but who’s really funding the studies? Big Pharma owns the reference drugs AND the biosimilars. It’s all one big loop. The Purple Book? Just a PR tool. They want you to believe switching won’t hurt you-but what about the long-term immune effects they’re not publishing? 🤔
Alex Lopez January 2, 2026
Ah yes, the FDA’s ‘highly similar’ standard. Let me guess-95% similarity is good enough, but if your protein folds at a 3.2-degree angle, you’re out? 🤦♂️ Meanwhile, the real cost savings are being blocked by patent trolls. Brilliant strategy, guys. Just make the science sound complicated so nobody notices the real issue.
Paula Alencar January 2, 2026
It’s critical to recognize that biosimilars are not just economic tools-they are equity tools. For patients in underserved communities, access to biologics has historically been a luxury. The approval of interchangeable biosimilars represents a profound shift toward healthcare justice. Every pharmacist who substitutes without hesitation is participating in a quiet revolution. We must champion this-not just tolerate it.
Gerald Tardif January 4, 2026
I’ve worked in pharma for 18 years. Biosimilars? They’re the real deal. The testing’s brutal-way harder than generics. You think it’s easy to match a protein that wobbles like a Jell-O mold? Nah. But when you see a kid with Crohn’s get their treatment for $300 instead of $3k? That’s the win.
Monika Naumann January 4, 2026
America spends billions on these so-called biosimilars while India produces life-saving generics at 1/10th the cost. Why does the FDA insist on such an over-engineered, bloated process? It’s not science-it’s protectionism disguised as regulation. We should be exporting our expertise, not locking patients behind bureaucratic walls.
Elizabeth Ganak January 6, 2026
i just got switched to a biosimilar last month and honestly? no difference. my joints still hurt the same but my bank account is happy 😊
Satyakki Bhattacharjee January 7, 2026
If you trust the FDA, you trust the system. If you trust the system, you trust the money. If you trust the money, you are not free. Biosimilars are the opiate of the masses. They give you hope while the real cure-transparency-is buried under patents and profit.
Kishor Raibole January 9, 2026
The FDA’s reliance on analytical comparability is a dangerous precedent. By allowing the substitution of complex biological entities based on molecular fingerprints alone, the agency has effectively outsourced clinical judgment to algorithms and corporate labs. This is not science. This is industrialized medicine-cold, calculated, and devoid of human nuance.
Liz MENDOZA January 9, 2026
To everyone saying biosimilars are risky-have you talked to the patients who’ve used them for years? I’ve seen people cry because they could finally afford their treatment. That’s not a corporate trick. That’s compassion in action.
Anna Weitz January 10, 2026
They say no new safety signals but what about the silent ones? The ones that show up after 5 years? The ones that get buried in databases no one checks? The FDA’s post-market surveillance is a joke. They monitor like a security camera with a broken lens