
What Are Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis?
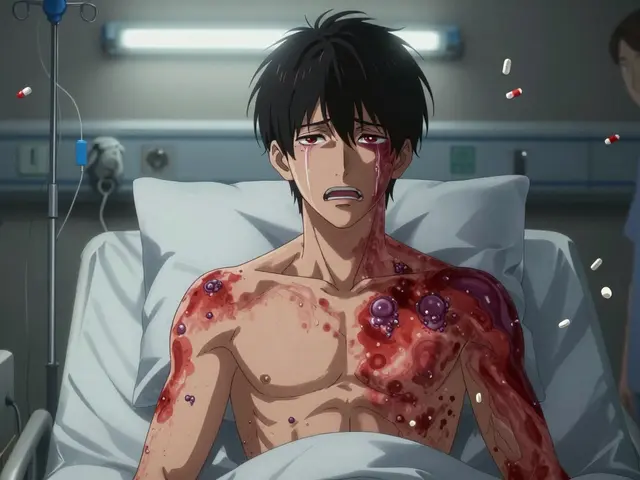
Stevens-Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis (TEN) are rare but deadly skin reactions triggered by medications. They don’t start with a simple rash-they begin like the flu. Fever, sore throat, fatigue, and burning eyes come on suddenly. Within a day or two, a red or purple rash spreads across the body. Blisters form. The top layer of skin starts to die and peel off, sometimes in sheets. This isn’t a bad sunburn. It’s a full-thickness skin breakdown, and it can affect your mouth, eyes, genitals, and throat.
SJS and TEN exist on a spectrum. If less than 10% of your skin detaches, it’s classified as SJS. If more than 30% is affected, it’s TEN. Between 10% and 30%? That’s overlap syndrome. The more skin involved, the higher the risk of death. In SJS, about 5% of people die. In TEN, that number jumps to over 30%. The difference isn’t just severity-it’s survival.
Which Medications Cause These Reactions?
These reactions don’t happen randomly. They’re tied to specific drugs. The most common culprits include:
- Allopurinol (used for gout)
- Lamotrigine (for epilepsy and bipolar disorder)
- Carbamazepine and phenytoin (anti-seizure meds)
- Nevirapine (an HIV drug)
- Piroxicam and meloxicam (NSAIDs for pain)
- Sulfamethoxazole (an antibiotic, often in Bactrim)
- Phenobarbital
It’s not just the drug itself. Cross-reactivity is real. If you had SJS from lamotrigine, you’re at high risk if you take carbamazepine or phenytoin-even if you’ve never taken them before. The same goes for sulfa drugs: if one caused a reaction, others in the same family could too. This is why doctors ask about past rashes before prescribing new meds.
These reactions can happen anytime-during treatment or even weeks after stopping the drug. Some people get sick after just a few days. Others don’t notice symptoms until they’ve been off the medication for over a week. That’s why monitoring doesn’t stop when the prescription ends.
Who’s at Higher Risk?
Not everyone who takes these drugs gets SJS or TEN. But some people are more vulnerable. Risk factors include:
- Having HIV or a weakened immune system from chemotherapy
- Having had a rash from an epilepsy drug before
- Being allergic to trimethoprim (a common antibiotic)
- Taking sodium valproate along with lamotrigine-this combo raises risk significantly
- Having a close family member who had SJS or TEN-this suggests a genetic link
- Starting lamotrigine too fast or restarting it after a break without slowly building back up
Children are more likely to develop SJS than adults, though it can happen at any age. If you’ve had this reaction once, your risk of it happening again is extremely high. Re-exposure to the same drug-or even similar ones-can trigger a faster, deadlier reaction.

What Does It Look Like?
The early signs are easy to miss. You might think you’ve got the flu. But here’s what separates SJS/TEN from a normal illness:
- Flu-like symptoms for 1-3 days
- Then: a painful red or purple rash that spreads fast
- Blisters forming on skin and mucous membranes
- Sores in your mouth, eyes, or genitals
- Skin that peels off with light pressure-like a burn
Doctors diagnose it with a skin biopsy. Under the microscope, they see full-thickness death of the epidermis-no inflammation, just dead skin. That’s the hallmark. Blood tests and imaging can’t confirm it. Only a biopsy can.
If you’re on lamotrigine and get a rash, don’t wait. Don’t assume it’s ‘just a side effect.’ Most rashes from lamotrigine are harmless. But if it’s spreading, blistering, or affecting your mouth or eyes? Go to A&E immediately. Delaying by even 24 hours can make the difference between life and death.
How Is It Treated?
There’s no magic cure. Treatment is about stopping the damage and supporting the body while it heals.
- Stop the drug immediately. This is non-negotiable. Even if you’re not sure which drug caused it, all suspect medications are pulled.
- Admit to hospital. Not a regular ward. Burn unit. ICU. These patients need the same care as major burn victims-fluids, infection control, pain management, wound care.
- Supportive care. IV fluids, nutrition through a tube if the mouth is too sore to eat, eye drops to prevent corneal damage, mouth rinses for ulcers.
- Immunomodulators? Some hospitals try steroids or IVIG (intravenous immunoglobulin), but evidence is mixed. No treatment has been proven to reliably save lives.
Time is everything. The sooner the drug is stopped and care begins, the better the outcome. Waiting even a day increases the chance of sepsis, organ failure, or death.
What Happens After You Survive?
Surviving SJS or TEN doesn’t mean you’re back to normal. Long-term damage is common-and often permanent.
- Eyes: 30-50% of survivors have lasting eye problems-dryness, light sensitivity, scarring, fused eyelids, or even blindness.
- Skin: Scarring, dark or light patches, permanent hair loss, and nail loss or deformity.
- Mouth and throat: Chronic dry mouth, gum disease, difficulty swallowing, esophageal narrowing.
- Genitals: Women may develop vaginal scarring and stenosis; men may face phimosis.
- Lungs and organs: Some develop pulmonary fibrosis, kidney damage, or heart complications.
Recovery takes months. Some people need years of follow-up with dermatologists, ophthalmologists, and gynecologists or urologists. Ocular complications require monitoring for at least a year-even if your eyes feel fine.

How Can You Prevent It?
Prevention starts with awareness.
- If you’re prescribed lamotrigine, carbamazepine, or allopurinol, ask your doctor about your risk. Tell them if you’ve had rashes before.
- Never start or increase the dose of high-risk meds quickly. Lamotrigine must be titrated slowly-rushing it is a known trigger.
- Don’t restart a drug after stopping it, even for a few days, without medical guidance. That’s a major red flag for SJS.
- During the first 3 months of taking high-risk meds, avoid new foods or medications. New triggers can confuse the symptoms.
- Know the warning signs. If you get a rash with fever and blistering, go to emergency care. Don’t wait. Don’t call your GP. Go to A&E.
These reactions are rare-fewer than five cases per million users per week. But when they happen, they’re catastrophic. That’s why vigilance matters.
What Should You Do If You Suspect SJS or TEN?
Act fast. Here’s your checklist:
- Stop taking all non-essential medications immediately.
- Do not wait for an appointment. Go to the nearest emergency department.
- Bring your medication list-every pill, supplement, and cream you’ve taken in the last 4 weeks.
- Do not apply creams, lotions, or ointments to the rash. This can make it worse.
- Keep your eyes and mouth moist with water or saline. Avoid rubbing.
- Do not assume it’s ‘just a rash.’ If skin is peeling or mucous membranes are involved, treat it as a medical emergency.
There’s no home remedy. No over-the-counter solution. This is not something you can wait out.
Final Thought: It’s Not About Fear-It’s About Awareness
These conditions are terrifying. But they’re preventable-if you know the signs. Millions take lamotrigine, allopurinol, and sulfamethoxazole every day without issue. Most rashes are harmless. But one wrong assumption can cost you everything.
If you’re on a high-risk medication, know the symptoms. Talk to your doctor. Keep a list of your drugs. And if something feels off-go to the hospital. Not tomorrow. Not next week. Now.
Can Stevens-Johnson Syndrome be cured?
There’s no cure for SJS or TEN. Treatment focuses on stopping the reaction, preventing complications, and supporting the body as it heals. Recovery depends on how quickly the trigger is removed and how much skin is affected. Many people survive, but long-term damage is common.
Is Stevens-Johnson Syndrome contagious?
No, SJS and TEN are not contagious. They’re immune-mediated reactions to medications, not infections. You can’t catch it from someone else.
Can you get SJS from over-the-counter drugs?
Yes. NSAIDs like piroxicam and meloxicam, which are available without a prescription, have been linked to SJS. Even common painkillers can trigger it in rare cases, especially if taken at high doses or for long periods.
How long after starting a drug can SJS develop?
Most cases appear within the first 8 weeks of starting a drug. But reactions can occur up to two weeks after stopping the medication. This is why monitoring doesn’t end when you finish your prescription.
If I had SJS once, can I take the same drug again?
Never. Re-exposure to the same drug-even in tiny amounts-can trigger a faster, more severe reaction, often fatal. You must avoid not only the original drug but also similar ones in the same chemical family.
Are there genetic tests to predict SJS risk?
Yes, for some drugs. For example, people of Asian descent taking carbamazepine are often tested for the HLA-B*15:02 gene variant, which increases risk. Testing isn’t routine everywhere, but if you’re prescribed high-risk meds, ask if genetic screening is available.
Can SJS affect children differently than adults?
Children are more likely to develop SJS than adults, especially when taking anticonvulsants or antibiotics. But the symptoms and progression are similar. The key difference is that children may not be able to describe symptoms like eye pain or mouth sores clearly, making early detection harder.
What should I do if I’m prescribed a high-risk drug?
Ask your doctor: Is this drug necessary? Are there safer alternatives? What are the warning signs? Get a written list of symptoms to watch for. Never start or increase the dose without medical supervision. Keep your medication list updated and share it with every healthcare provider.






Matt W February 2, 2026
Just had my sister go through this with lamotrigine. She thought it was a bad allergy until her mouth started peeling. Got to the ER in time, but spent 3 weeks in the burn unit. Never take a rash from these meds lightly. I now keep a printed list of warning signs taped to my fridge.
Anthony Massirman February 2, 2026
Stop. Drop. Go to A&E. That’s it.
George Firican February 4, 2026
It’s staggering how many people treat these drugs like candy. Allopurinol for gout? Sure, why not. Lamotrigine for mood swings? Easy fix. But behind every statistic is someone who lost skin, sight, or breath because someone assumed it was ‘just a rash.’ We’ve normalized risk in medicine until it’s no longer a risk-it’s a waiting game. The body doesn’t negotiate. It doesn’t care if you’re busy, tired, or thought you were being careful. One wrong pill, one skipped taper, one ignored blister-and the cascade begins. And then you’re in a hospital bed wondering why no one warned you that your immune system doesn’t do ‘maybe.’ It does absolute. And it doesn’t forgive.
Vatsal Srivastava February 6, 2026
Everyone panics about meds but ignores that 99% of people take these drugs fine. You’re more likely to get hit by lightning than get SJS. Stop fearmongering
Solomon Ahonsi February 7, 2026
So what? You want us to stop taking all meds? You’re just scaring people for clicks. My uncle took carbamazepine for 20 years and never had a problem. This post is just fear porn.
Brett MacDonald February 8, 2026
bro i had a rash once after taking meloxicam and i just took benadryl and it went away in 2 days. why are people so extra these days
jay patel February 10, 2026
lol so you're telling me if i take a single pill of lamotrigine and get a tiny red spot on my arm i need to book a flight to the burn unit? my grandma took phenobarbital for 40 years and still danced at weddings. maybe the real issue is that we've turned every minor symptom into a death sentence. also why does everyone act like the skin is the only thing that matters? i once had a rash from amoxicillin and it was way more annoying than the actual infection. also hla testing? that's just expensive overkill unless you're in a lab coat and not a human being trying to live their life.
larry keenan February 11, 2026
While the clinical presentation and mortality statistics are well-documented, the generalization of cross-reactivity across drug classes warrants further scrutiny. The immunogenetic underpinnings-particularly HLA-B*15:02 association in Southeast Asian populations-are not universally applicable, and blanket avoidance strategies may lead to therapeutic nihilism in populations where genetic screening is inaccessible. Additionally, the efficacy of IVIG remains inconclusive in randomized controlled trials, and current guidelines are largely consensus-based rather than evidence-driven. The emphasis on immediate discontinuation is valid, but the lack of standardized diagnostic criteria outside biopsy may lead to overdiagnosis in primary care settings.
Ansley Mayson February 11, 2026
Why do Americans turn every drug reaction into a crisis? In my country we just wait it out. If you get a rash, you’re weak. This post is just another way to make people paranoid about medicine. Stop giving out free anxiety.